
Table of Contents >> Show >> Hide
- What You’ll Learn
- Diagnosis vs. Suspicion: The Two-Step Reality
- Signs & Symptoms of Testicular Cancer
- Not Every Lump Is Cancer (But Every New Lump Deserves a Look)
- How Doctors Diagnose Testicular Cancer: Step-by-Step
- Why Doctors Usually Avoid Needle Biopsy
- How to Prep for Your Appointment (So You Don’t Forget Everything Under Pressure)
- Testicular Self-Exam & Screening: The Nuanced Truth
- What Happens After a Diagnosis (A Quick Look Ahead)
- FAQs: Quick Answers to Common (Very Human) Questions
- Experiences Related to Diagnosing Testicular Cancer (What It Can Feel Like)
- 1) “I thought it was nothing because it didn’t hurt.”
- 2) The ultrasound feels awkward… but it’s fast and straightforward.
- 3) Tumor marker tests can be emotionally confusing.
- 4) The phrase “remove the testicle” lands like a brickthen you start wanting details.
- 5) Waiting is frequently the hardest part.
- Conclusion
Testicular cancer is one of those topics that can make even the bravest adult suddenly feel like a nervous middle-schooler in health class.
The good news: it’s highly treatable, especially when caught early. The tricky part: your body doesn’t always send a flashing neon sign that says,
“Hello, I am a serious medical issue.” Sometimes it sends… a small lump and a vague sense of “huh.”
This guide walks through the signs and symptoms of testicular cancer, what doctors do to confirm a diagnosis,
and what to do if you notice a change. It’s educationalnot a substitute for medical care.
If something feels off, a clinician (often a urologist) is the right next step.
Diagnosis vs. Suspicion: The Two-Step Reality
When people say “How do I diagnose testicular cancer?” what they usually mean is:
How do I know if this change is something I should take seriously?
Here’s the honest translation:
-
You can’t confirm a diagnosis at home (no matter how confident you are in your Googling skills).
But you can notice changes early. -
Clinicians diagnose testicular cancer using a physical exam, scrotal ultrasound, blood tumor marker tests,
and (when needed) surgery to remove the testicle for definitive pathology.
So think of this article as your “Should I get this checked?” and “What will the doctor do next?” playbook.
Signs & Symptoms of Testicular Cancer
The most common early sign
The classic early warning sign is a new lump or swelling in one testicle.
Many testicular tumors are painless, which is why they can be easy to ignore.
Other common symptoms
- Heaviness in the scrotum (like your underwear suddenly got upgraded to “weighted”)
- Dull ache in the lower abdomen or groin
- Enlargement of one testicle or a noticeable change in shape/firmness
- Discomfort or pain in the testicle or scrotum (less common, but it happens)
- Sudden fluid buildup in the scrotum
Less common symptoms (still important)
- Breast tenderness or enlargement (gynecomastia). Some tumors affect hormones, which can lead to breast changes.
- Back pain (can happen if cancer spreads to lymph nodes in the abdomen)
When to seek urgent care
Sudden, severe testicular pain is a medical emergency until proven otherwise (testicular torsion is one reason).
If pain comes on fast and intense, don’t wait for a “see how it feels tomorrow” experimentget urgent evaluation.
One more reality check: it’s normal for one testicle to hang lower or be slightly larger than the other.
What’s not “normal” is a new change that wasn’t there before.
Not Every Lump Is Cancer (But Every New Lump Deserves a Look)
Finding something new can trigger instant panic. But many scrotal or testicular lumps come from conditions that are
not cancer.
Common non-cancer explanations doctors consider
- Epididymal cyst or spermatocele (often a smooth bump near the top/back of the testicle)
- Hydrocele (fluid around the testiclemore “water balloon” than “solid lump”)
- Varicocele (enlarged veinsoften described as “a bag of worms” in the scrotum)
- Infection/inflammation (epididymitis or orchitisoften painful and may come with urinary symptoms)
- Hernia (a bulge that may change with standing/straining)
This is exactly why a scrotal ultrasound is so helpful: it can show whether a lump is
inside the testicle (more concerning for cancer) or outside it (often benign).
How Doctors Diagnose Testicular Cancer: Step-by-Step
If you see a clinician for a testicular lump or scrotal swelling, the goal is to answer two questions:
(1) What is it? and (2) Has it spread?
Step 1: Medical history and physical exam
The exam includes checking the testicles and scrotum, plus nearby areas like the abdomen and lymph nodes.
Clinicians look for size differences, firmness, tenderness, and the exact location of any mass.
Step 2: Scrotal ultrasound (the MVP test)
A scrotal ultrasound uses sound waves to create images of the testicle and surrounding structures.
It’s painless, quick, and extremely useful for identifying a suspicious solid intratesticular mass.
Ultrasound can also help distinguish cancer from other causes of swelling.
Step 3: Blood tests for tumor markers
If cancer is suspected, clinicians typically order blood tests for the main testicular tumor markers:
- AFP (alpha-fetoprotein)
- beta-hCG (beta human chorionic gonadotropin)
- LDH (lactate dehydrogenase)
Important nuance: tumor markers can support the diagnosis and help with staging and follow-up,
but they don’t confirm cancer by themselves. Levels can be normal even when cancer is present,
and some markers can rise for reasons unrelated to testicular cancer. They’re cluesuseful clues, but still clues.
Another key detail: pure seminoma typically does not raise AFP. If AFP is elevated, clinicians often suspect
a nonseminomatous germ cell tumor component. (Yes, this is the part where medicine becomes a taxonomy game.)
Step 4: Imaging to check for spread (staging)
If tests suggest testicular cancer, the next step is often imaging to look for metastasisespecially to lymph nodes in the abdomen
and to the lungs. Depending on the situation, clinicians may order:
- CT scan of the abdomen and pelvis
- Chest imaging (often a chest X-ray or CT)
The exact set of imaging tests can vary based on the clinical picture, tumor markers, and ultrasound findings.
Step 5: Surgery to confirm diagnosis (inguinal orchiectomy)
Here’s the part that surprises many people: when testicular cancer is strongly suspected, doctors typically confirm the diagnosis
by removing the affected testicle through an incision in the groin (an inguinal orchiectomy),
then examining the tissue under a microscope.
That sounds dramaticand emotionally it can bebut it’s also the standard approach because it both
diagnoses and often treats cancer that’s limited to the testicle.
Why Doctors Usually Avoid Needle Biopsy
For many cancers, a needle biopsy is the normal first step. Testicular cancer is different.
Needle biopsy is generally avoided because of concerns about altering lymphatic drainage pathways and the theoretical risk of spreading tumor cells.
That’s why the typical “biopsy” is actually the surgical removal of the testicle via the groin route when cancer is suspected.
How to Prep for Your Appointment (So You Don’t Forget Everything Under Pressure)
If you’re heading in to get evaluated for a testicular lump, you don’t need to arrive with a medical degree.
But a little prep can help.
What to note beforehand
- When you first noticed the change
- Whether it’s getting bigger, changing shape, or staying the same
- Any pain (and whether it’s sudden vs. gradual)
- Swelling, heaviness, or fluid buildup
- Symptoms elsewhere: back pain, cough, shortness of breath, unexplained weight loss, breast tenderness
- Relevant history: undescended testicle, prior testicular cancer, family history
Questions worth asking
- “Based on the exam, what are the most likely causes?”
- “Do I need a scrotal ultrasound?”
- “Should we check tumor markers (AFP, beta-hCG, LDH)?”
- “If this looks suspicious, what’s the next step and how fast should it happen?”
- “Should I see a urologist?”
- “If surgery is needed, what about fertility preservation or sperm banking?”
Pro-tip: bring a note on your phone. In a stressful appointment, even the most organized person can forget their own ZIP code.
Testicular Self-Exam & Screening: The Nuanced Truth
You’ll find conflicting advice about routine monthly testicular self-exams.
That’s because major organizations differ in emphasis, and evidence that routine screening reduces death is limited.
What experts generally agree on
- There is no standard routine screening test for testicular cancer in people without symptoms.
-
Some organizations do not recommend routine self-exam for everyone, while others encourage self-awareness or optional monthly checks
especially if you’re at higher risk. -
Regardless of how often you self-check, the most important point is this:
don’t ignore a new lump or change.
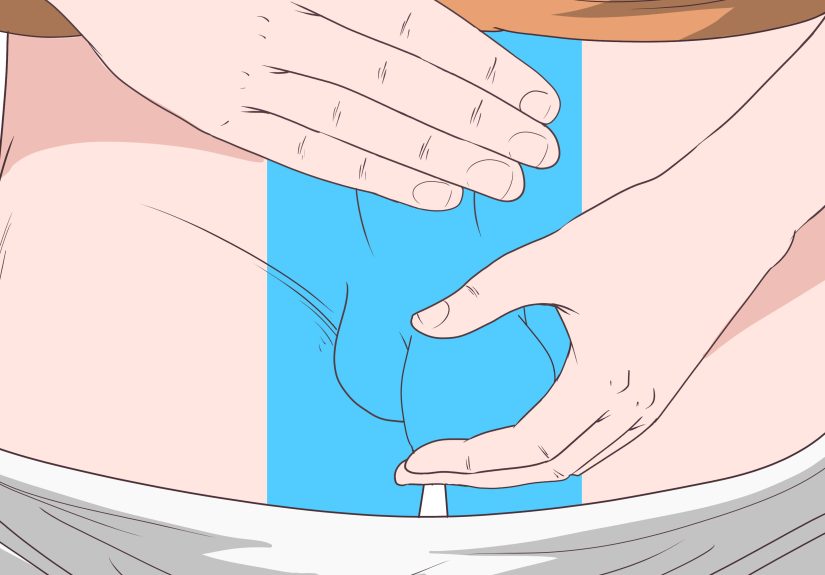
If you choose to self-check (a simple method)
- Do it after a warm shower when the scrotal skin is relaxed.
- Check each testicle separately, gently rolling it between your fingers and thumb.
- Feel for a new hard lump, a change in size, or a change in firmness.
- Know the normal “bumps”: the epididymis (a soft, cord-like structure) sits along the back/top of the testicle.
- If something feels new or concerning, schedule a medical evaluation.
If you have higher risk factors (like a history of undescended testicle), talk with a clinician about what monitoring makes sense for you.
The right approach is the one that balances awareness without turning every Tuesday into a panic festival.
What Happens After a Diagnosis (A Quick Look Ahead)
Once pathology confirms testicular cancer, clinicians classify the tumor type (commonly seminoma or
nonseminomatous germ cell tumor) and determine the stage using imaging and tumor markers.
Treatment plans may include surveillance, chemotherapy, radiation (more commonly for certain seminomas), or surgery for lymph nodes,
depending on the details.
If fertility is a concern, ask early about sperm bankingideally before treatment beyond orchiectomy.
FAQs: Quick Answers to Common (Very Human) Questions
“Does testicular cancer hurt?”
Often, no. Many people notice a painless lump or swelling. Pain can happen, but it’s not required for something to be serious.
“Can I have normal tumor markers and still have cancer?”
Yes. Tumor markers can be helpful, but not every tumor produces them at detectable levels.
That’s why ultrasound and pathology matter.
“What if it’s just swelling and no lump?”
Swelling, fluid buildup, or a heavier feeling can still warrant evaluationespecially if it’s new or persistent.
“Who gets testicular cancer?”
It’s most common in younger and middle-aged men, but it can occur at other ages too.
Risk factors include an undescended testicle, personal or family history, and certain genetic or health factors.
“Is losing a testicle the end of… everything?”
No. Many people live normal lives after orchiectomy, including normal sexual function and fertility (depending on the other testicle and treatment).
Your care team can discuss testosterone, fertility, and prosthesis options if you want them.
Experiences Related to Diagnosing Testicular Cancer (What It Can Feel Like)
The stories below are composites based on common experiences people report in clinical settings and patient education materials.
They’re meant to make the process feel less mysteriousnot to replace medical advice.
1) “I thought it was nothing because it didn’t hurt.”
A lot of people expect cancer to announce itself with pain. Testicular cancer often doesn’t.
One of the most common real-life patterns is someone finding a small, firm lump and ignoring it because it’s painless.
Days turn into weeks. Weeks become months. Then a partner notices a size difference, or the person finally admits,
“Okay, this has definitely been here for a while.”
The lesson isn’t “panic sooner.” It’s “don’t rely on pain as your personal health alarm system.”
A painless lump is still worth a prompt check.
2) The ultrasound feels awkward… but it’s fast and straightforward.
People often worry the ultrasound will be painful or invasive. Usually, it’s neither. It’s more like:
gel, gentle pressure, a wand, and a lot of silent internal commentary like, “So this is my life now.”
The technician may not tell you results on the spot (policy varies), which can be frustrating.
But the ultrasound itself is typically quickand incredibly informative for doctors deciding what to do next.
3) Tumor marker tests can be emotionally confusing.
Blood tests sound simple, but the meaning can be complicated.
Some people feel relief when tumor markers come back normalthen feel whiplash when the clinician says,
“We still need to take this seriously.” Others see elevated numbers and assume the worst immediately.
In reality, tumor markers are pieces of a puzzle. Elevated markers can support suspicion and help with staging,
but they’re not a stand-alone verdict. Normal markers don’t automatically clear you either.
Most people feel better when the care team explains what each marker can and can’t tell you.
4) The phrase “remove the testicle” lands like a brickthen you start wanting details.
When orchiectomy enters the conversation, many people go numb for a moment.
The fear isn’t only about cancerit’s also about identity, sex, fertility, and “What happens to me after this?”
This is where clear, practical information helps:
- It’s commonly a same-day surgery.
- It’s done through the groin, not by cutting the scrotum.
- It often confirms the diagnosis and can be curative if the cancer is localized.
- Many people do well with one testicle, and options exist if you want a prosthesis.
People often report that once they understand the “why” behind the approach, the plan feels less like a nightmare
and more like a route forward.
5) Waiting is frequently the hardest part.
The waitingbetween noticing a symptom and getting an appointment, between the ultrasound and the report,
between surgery and pathologycan feel longer than it actually is.
Many people describe their brain doing Olympic-level catastrophizing at 2:00 a.m.
What helps, in real-world terms:
writing down questions, bringing a trusted person to appointments if possible,
and focusing on the next concrete step (“ultrasound Tuesday,” “urologist Thursday”) instead of the entire future at once.
Bottom line: noticing a change early and getting evaluated promptly is the move. It’s not overreacting.
It’s the health equivalent of putting on a seatbeltsimple, practical, and very much in your favor.





