
Table of Contents >> Show >> Hide
- When Chest Pain Feels Like a Heart Attackbut Isn’t
- Heart Attack Warning Signs You Should Not Ignore
- Why Noncardiac Chest Pain Can Feel So Real
- Common Conditions That Mimic a Heart Attack
- How Doctors Tell the Difference
- Risk Factors That Raise Concern
- What to Do During Chest Pain
- Prevention and Everyday Habits That May Help
- Experience-Based Reflections: Living Through Chest Pain Scares
- Conclusion: Respect Chest Pain, Even When It Is Not a Heart Attack
- SEO Tags
Important note: This article is for educational purposes only. Chest pain can be harmless, serious, or life-threatening. If you have new, severe, unexplained, or persistent chest painespecially with shortness of breath, sweating, nausea, faintness, or pain spreading to the arm, jaw, neck, back, or stomachcall 911 or seek emergency medical care immediately.
When Chest Pain Feels Like a Heart Attackbut Isn’t
Chest pain has a special talent for ruining an otherwise normal Tuesday. One minute you are folding laundry, climbing stairs, eating tacos, or trying to convince yourself that “just one more email” counts as productivity. The next minute, there is a tight, burning, stabbing, squeezing, or mysterious “what on earth is happening in there?” feeling in your chest.
The scary part is that chest pain can mimic a heart attack even when the heart is not the source of the problem. Acid reflux can burn behind the breastbone. Inflamed rib cartilage can produce sharp pain. Panic attacks can feel like the body’s alarm system got stuck on maximum volume. Lung problems, esophageal spasms, gallbladder trouble, and muscle strain can also create chest discomfort that looks suspiciously cardiac from the outside.
But here is the golden rule: never try to diagnose dangerous chest pain by vibes alone. Even doctors do not simply glance across the room and declare, “Relax, it’s probably your sandwich.” They use a history, exam, electrocardiogram, blood tests, imaging, and clinical judgment to rule out emergencies. That is why the safest first step with concerning chest pain is medical evaluation.
Heart Attack Warning Signs You Should Not Ignore
A heart attack happens when blood flow to part of the heart muscle is blocked. The classic symptom is pressure, squeezing, tightness, heaviness, or pain in the center or left side of the chest. It may last more than a few minutes, disappear, and return. Some people describe it as an elephant sitting on the chest; others say it feels like bad indigestion with a side of dread.
Common heart attack symptoms
Symptoms may include chest discomfort, pain spreading to one or both arms, the back, neck, jaw, shoulder, teeth, or upper belly, shortness of breath, cold sweat, nausea, vomiting, lightheadedness, unusual fatigue, or a sudden sense that something is very wrong.
Symptoms can be different in women, older adults, and people with diabetes
Not everyone gets dramatic movie-style chest pain. Women may have chest discomfort, but they are also more likely to report shortness of breath, nausea, upper back pressure, jaw pain, extreme fatigue, or indigestion-like symptoms. Older adults and people with diabetes may have subtle symptoms because nerve function and pain perception can differ. Translation: if your body whispers instead of shouts, listen anyway.
If symptoms are sudden, severe, unusual, or paired with breathlessness, sweating, faintness, or radiating pain, do not wait to see whether it “settles down.” Call emergency services. Driving yourself is not a heroic move; it is a risky one.
Why Noncardiac Chest Pain Can Feel So Real
Noncardiac chest pain means chest pain that is not caused by the heart. The phrase sounds reassuring, but the experience may feel anything but reassuring. Many structures share the chest neighborhood: the esophagus, lungs, ribs, muscles, nerves, gallbladder, stomach, and major blood vessels. They all send signals through nerves that can overlap, blur, and confuse the brain.
That is why acid reflux can feel like heart pain, a strained chest muscle can feel alarming, and anxiety can create physical symptoms that seem impossible to “just be stress.” Your body is not being dramatic. It is using a very noisy communication system, and sometimes every department sends the same memo: “Chest problem!”
Common Conditions That Mimic a Heart Attack
1. GERD and acid reflux
Gastroesophageal reflux disease, better known as GERD, is one of the most common causes of noncardiac chest pain. It happens when stomach acid flows back into the esophagus, the tube connecting the mouth and stomach. Because the esophagus runs through the chest, irritation there can create burning, pressure, or pain behind the breastbone.
GERD-related chest pain often appears after eating, when lying down, after a heavy meal, or after spicy, fatty, acidic, or caffeinated foods. It may come with sour-tasting fluid in the throat, burping, throat clearing, hoarseness, cough, nausea, or trouble swallowing. However, GERD does not always announce itself with classic heartburn, which is why it can be a master impersonator.
Example: A person eats a large late-night dinner, lies down to watch television, then feels burning pressure in the chest. It improves after sitting upright or taking an antacid. That pattern suggests reflux, but if the pain is new, severe, or comes with shortness of breath or sweating, it still needs urgent evaluation.
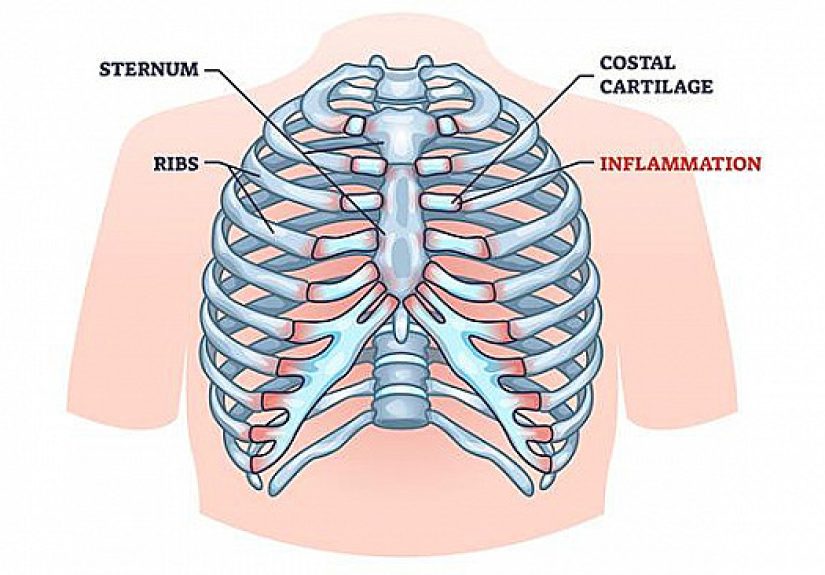
2. Costochondritis
Costochondritis is inflammation of the cartilage where the ribs attach to the breastbone. It can cause sharp, aching, or pressure-like pain in the front of the chest. The pain may worsen with deep breathing, coughing, twisting, lifting, or pressing on the sore area.
This condition can follow heavy lifting, intense exercise, repeated coughing, physical strain, or sometimes no obvious trigger at all. The good news is that costochondritis is usually not dangerous. The annoying news is that it can feel terrifyingly close to heart pain.
One clue is tenderness: if pressing on a specific spot near the breastbone reproduces the pain, a chest wall cause becomes more likely. Still, tenderness does not automatically rule out heart disease, especially in people with risk factors or new symptoms.
3. Muscle strain
Chest muscles can become strained after workouts, moving furniture, shoveling snow, carrying heavy bags, coughing hard, or doing an ambitious home project that began with “How hard could it be?” Muscle pain often feels worse with certain movements, stretching, reaching, or pressing on the area.
Musculoskeletal chest pain may improve with rest, heat, gentle stretching, or anti-inflammatory medicine when appropriate. But because muscle strain and heart-related pain can overlap, new or unexplained chest pain deserves caution.
4. Panic attacks and anxiety
A panic attack can cause chest tightness, racing heartbeat, shortness of breath, trembling, sweating, dizziness, nausea, tingling, and a sudden fear of losing control. In other words, it can feel very much like a medical emergency.
Panic-related chest pain may come on suddenly, peak within minutes, and occur during emotional stressor seemingly out of nowhere. The pain may be sharp, tight, or centered in one area. But because panic attacks and heart attacks can share symptoms, first-time chest pain or severe symptoms should be evaluated medically before assuming anxiety is the cause.
5. Esophageal spasm
The esophagus normally moves food toward the stomach through coordinated muscle contractions. Sometimes those contractions become abnormal or intense, creating chest pain that can feel like squeezing pressure. Esophageal spasm may occur with difficulty swallowing, the sensation of food getting stuck, or pain triggered by very hot or cold drinks.
This is one reason digestive causes can be so confusing. The esophagus sits close to the heart, and its pain signals can mimic angina. A doctor may consider reflux treatment, swallowing studies, endoscopy, or other tests depending on symptoms.
6. Lung-related chest pain
Lung problems can also create chest pain. Pneumonia may cause fever, cough, fatigue, and chest discomfort. Pleurisy, inflammation of the lining around the lungs, often causes sharp pain that worsens with breathing or coughing. A pulmonary embolism, which is a blood clot in the lung, can cause sudden chest pain, shortness of breath, rapid breathing, fast heart rate, faintness, or coughing blood. A collapsed lung can cause sudden one-sided chest pain and trouble breathing.
These conditions are not “heart attacks,” but some can be emergencies. Chest pain with sudden breathlessness should be taken seriously every time.
7. Gallbladder and digestive conditions
Gallstones, gastritis, ulcers, pancreatitis, and other digestive issues can create upper abdominal pain that radiates into the chest, back, or shoulder. Gallbladder pain often appears after a fatty meal and may settle under the right ribs or right shoulder blade. Ulcer pain may burn or gnaw and may change with eating.
Digestive pain can be sneaky because it lives near the lower chest and upper abdomen, a region where people are not always sure which organ is filing the complaint. When in doubt, let a clinician sort it out.
8. Pericarditis
Pericarditis is inflammation of the sac around the heart. It may cause sharp chest pain that improves when sitting up and leaning forward and worsens when lying down or taking a deep breath. It can follow viral infections and may come with fever or fatigue. Although it is different from a heart attack, it still involves the heart area and needs medical evaluation.
9. Aortic dissection
An aortic dissection is a tear in the inner layer of the aorta, the body’s main artery. It can cause sudden, severe chest or back pain sometimes described as tearing or ripping. This is a life-threatening emergency. If pain is abrupt, intense, or unlike anything felt before, call emergency services immediately.
How Doctors Tell the Difference
Because chest pain has many possible causes, clinicians start by ruling out dangerous conditions. The evaluation may include questions about the pain, medical history, risk factors, medications, recent illness, physical activity, meals, stress, and associated symptoms.
Tests that may be used
An electrocardiogram can look for changes in heart rhythm or signs of reduced blood flow. Blood tests such as troponin can detect heart muscle injury. Chest X-rays may help identify pneumonia, fluid, lung collapse, or other chest problems. Depending on the situation, doctors may order CT scans, stress testing, echocardiography, endoscopy, gallbladder imaging, or other studies.
The key point is that diagnosis is not based on one clue. It is based on the full pattern. A burning sensation after pizza points one way. Crushing pressure with sweating and jaw pain points another. Sharp pain when pressing the rib joint suggests something else. But medicine loves exceptions, so testing matters.
Risk Factors That Raise Concern
Chest pain deserves extra attention if you have risk factors for heart disease, including high blood pressure, high cholesterol, diabetes, smoking, obesity, kidney disease, a history of heart disease, a strong family history of early heart disease, or a sedentary lifestyle. Age also matters, though younger people are not magically immune.
Recent surgery, long travel, pregnancy, certain clotting disorders, cancer, or leg swelling may raise concern for blood clots. Fever and cough may suggest infection. Recent intense lifting may suggest muscle strain. A meal-related pattern may suggest reflux or gallbladder disease. Doctors use these details like puzzle pieces, except the puzzle is your chest and nobody wants to guess wrong.
What to Do During Chest Pain
Call 911 if symptoms suggest an emergency
Call emergency services for chest pressure, squeezing, heaviness, or pain that lasts more than a few minutes, goes away and returns, or appears with shortness of breath, cold sweat, nausea, faintness, weakness, confusion, or pain spreading to the arm, jaw, neck, back, shoulder, or stomach.
Do not drive yourself
If the pain could be a heart attack or other emergency, do not drive yourself unless there is truly no alternative. Emergency medical teams can begin evaluation and treatment on the way to the hospital.
Do not rely on internet diagnosis
A search engine can list possibilities, but it cannot listen to your heart, check oxygen levels, perform an ECG, or measure troponin. The internet is useful for learning; it is not a chest pain referee.
Track details if symptoms are mild and nonurgent
If a clinician has already ruled out an emergency and symptoms are mild or recurring, keep notes. Track when the pain happens, how long it lasts, what it feels like, whether it relates to meals, exercise, stress, position, breathing, or movement, and what makes it better or worse. This information can help your healthcare provider narrow the cause.
Prevention and Everyday Habits That May Help
Prevention depends on the cause. For reflux, it may help to avoid late-night heavy meals, reduce trigger foods, eat smaller portions, elevate the head of the bed, maintain a healthy weight, and follow medical advice about acid-reducing medication. For chest wall pain, proper lifting technique, gradual exercise progression, stretching, posture work, and rest after strain may help.
For anxiety-related symptoms, treatment may include cognitive behavioral therapy, breathing techniques, sleep improvements, exercise, mindfulness, and sometimes medication prescribed by a professional. For heart health, the big-ticket habits still matter: do not smoke, manage blood pressure, control cholesterol and blood sugar, move regularly, eat a balanced diet, and keep up with preventive care.
The goal is not to become afraid of every twinge. The goal is to respect chest pain enough to respond wisely.
Experience-Based Reflections: Living Through Chest Pain Scares
Anyone who has experienced chest pain that mimics a heart attack knows the emotional whiplash. The mind moves fast: “Is this heartburn? Did I pull something? Am I dying? Should I call someone? Why did I eat nachos at 10 p.m.?” Chest pain is not just a physical sensation; it is a full-body alarm that can turn even calm people into amateur detectives with shaky hands.
One common experience is the late-night reflux scare. A person eats a big dinner, adds coffee or chocolate, lies down, and then feels burning pressure behind the breastbone. The discomfort may climb toward the throat, come with a sour taste, and improve when sitting upright. After medical evaluation rules out heart trouble, the lesson becomes clear: the stomach has opinions, and it files complaints upward. Many people learn to avoid huge meals before bed, keep antacids or prescribed medication handy, and stop treating the couch like a digestive strategy.
Another familiar story involves costochondritis or muscle strain. Someone starts a new workout, lifts boxes, coughs for a week, or sleeps in a strange position. Then a sharp pain appears near the breastbone. Pressing the area hurts. Twisting hurts. Taking a deep breath may hurt. The fear is real because the pain is in the chest, but once a doctor rules out dangerous causes, the treatment may be surprisingly ordinary: rest, heat, gentle movement, and patience. The experience teaches humility. Apparently, one enthusiastic afternoon of “I can carry all the grocery bags at once” can have consequences.
Panic-related chest pain brings a different lesson. People often feel embarrassed when they are told anxiety may be involved, as if the pain was imaginary. It was not. Panic can produce real chest tightness, breathlessness, dizziness, and pounding heartbeat. The body’s stress response is powerful. After emergencies are ruled out, many people feel better understanding that anxiety is not “nothing.” It is a treatable condition with physical effects. Therapy, breathing practice, sleep routines, and medical support can make future episodes less frightening.
Some people describe a turning point after a chest pain evaluation: they finally take prevention seriously. They start checking blood pressure, schedule overdue appointments, walk more consistently, reduce smoking exposure, improve sleep, or learn their family history. A scary symptom becomes a wake-up callnot necessarily because something terrible happened, but because the body got their attention.
The best experience-based advice is simple: do not gamble with new chest pain. If it is severe, persistent, unusual, or paired with warning signs, get emergency help. If it turns out to be reflux, muscle strain, or anxiety, that is not a wasted trip; that is good news with documentation. Peace of mind is not silly. It is one of the most underrated treatments in health care.
Conclusion: Respect Chest Pain, Even When It Is Not a Heart Attack
Chest pain that mimics a heart attack can come from many sources, including GERD, costochondritis, muscle strain, panic attacks, lung conditions, esophageal spasms, gallbladder problems, or inflammation around the heart. Some causes are manageable and not life-threatening. Others require urgent care. The challenge is that symptoms overlap, and guessing can be dangerous.
The smartest approach is balanced: do not panic over every minor ache, but do not dismiss chest pain that is new, severe, persistent, or accompanied by red flags. When your chest sends a warning, listen first and analyze later. Your heart, lungs, ribs, stomach, and nervous system may all share the same neighborhood, but emergency care is how you find out who is actually knocking on the door.






