
Table of Contents >> Show >> Hide
- What Is Calcification in the Breast?
- Types of Breast Calcifications
- Common Causes of Calcification in Breast Tissue
- Do Breast Calcifications Cause Symptoms?
- How Doctors Diagnose and Evaluate Breast Calcifications
- Treatment for Calcification in Breast
- When Should You Be Concerned?
- Can Breast Calcifications Be Prevented?
- Frequently Asked Questions
- Experiences Many People Have With Breast Calcifications
- Conclusion
Finding out you have calcification in the breast can make your brain do what brains do best: panic first, ask questions second, and open about 37 imaginary worst-case tabs in the background. The good news is that breast calcifications are common, especially as people get older, and most of them are not cancer. In fact, many are simply tiny calcium deposits that show up on a mammogram and never cause symptoms, pain, or trouble.
Still, “most are benign” is not the same thing as “ignore it and go make a sandwich.” Some calcifications can be a clue that something unusual is happening in the breast tissue. That is why radiologists pay close attention to the pattern, size, shape, and distribution of these spots on imaging. A few white specks can be a boring non-event. A tight, irregular cluster can trigger a closer look.
This guide breaks down what breast calcifications are, the different types, common causes, how doctors decide whether they are harmless or suspicious, and what treatment may look like if follow-up testing finds a problem. If you want the short version, here it is: breast calcifications are usually a mammogram story, not a symptom story, and the “treatment” is often observation unless the pattern suggests precancer or cancer.
What Is Calcification in the Breast?
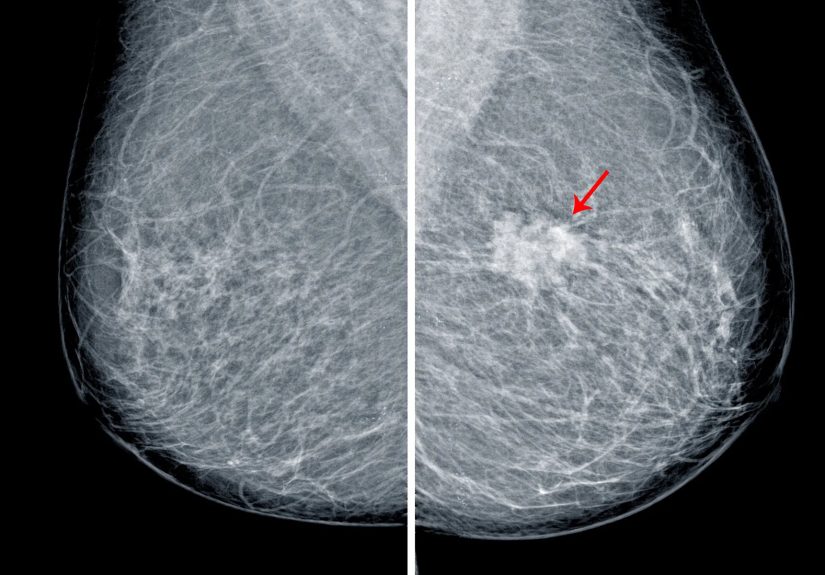
Breast calcifications are tiny deposits of calcium that form in breast tissue. They are too small to feel during a self-exam or a clinical breast exam, which is why they are usually discovered during a screening mammogram. On the image, they appear as bright white spots or flecks.
One important point that deserves a giant neon sign: breast calcifications are not caused by eating too much calcium, taking calcium supplements, or loving yogurt a little too enthusiastically. They are a tissue finding, not a dietary punishment. They also do not “turn into” cancer. Instead, they can act as markers that point to changes happening inside the breast.
Sometimes those changes are completely harmless, such as aging, past inflammation, or a benign cyst. Sometimes they are associated with abnormal cell growth, including ductal carcinoma in situ, also called DCIS, which is an early, non-invasive breast cancer found in the milk ducts.
Types of Breast Calcifications
Macrocalcifications
Macrocalcifications are the larger type. On a mammogram, they usually appear as coarse, round, or scattered white dots. Radiologists generally consider these benign. They are often linked to normal aging changes, old injury, inflammation, or other noncancerous processes in the breast. In many cases, macrocalcifications do not require extra testing beyond routine screening.
If macrocalcifications had a personality, they would be the neighbor who waves politely and minds their own business. They are common, often expected, and rarely dramatic.
Microcalcifications
Microcalcifications are much smaller. These tiny specks can also be benign, and often are. The reason they get more attention is not because they are tiny and mysterious, but because certain patterns of microcalcifications can be linked to precancerous changes or breast cancer.
Radiologists look closely at whether the microcalcifications are grouped together, arranged in a line, or have irregular shapes. A scattered pattern may be reassuring. A tight cluster or a suspicious line can raise concern and lead to more imaging or a biopsy.
Benign vs. Suspicious Patterns
When doctors evaluate calcifications, the pattern matters more than the mere fact that calcium is present. Breast imaging specialists often divide calcifications into broadly benign, probably benign, or suspicious categories. Clearly benign calcifications usually need no special treatment. Probably benign calcifications may need repeat imaging in about six months. Suspicious calcifications are more likely to lead to a biopsy.
This is why two people can both hear the phrase “breast calcifications” and end up on very different paths. One gets a routine annual mammogram and moves on with life. The other gets a call-back for magnified views and maybe a stereotactic biopsy. Same phrase, very different plot twist.
Common Causes of Calcification in Breast Tissue
Breast calcifications can happen for many reasons, and most of those reasons are benign. Common causes include:
- Normal aging changes in breast tissue
- Past breast injury or trauma
- Inflammation or previous infection, including mastitis
- Benign breast cysts
- Fibroadenomas and other noncancerous breast lumps
- Fibrocystic changes, including milk of calcium
- Mammary duct ectasia
- Changes after breast surgery or biopsy
- Radiation therapy to the breast
- Skin calcifications or calcifications in blood vessels
Less commonly, calcifications may be associated with abnormal cells or cancer. One of the best-known examples is DCIS, which is often first detected because suspicious microcalcifications appear on a mammogram before a lump can be felt. In some cases, invasive breast cancer may also be linked to calcification patterns, although many cancers appear as masses rather than calcifications.
So yes, calcifications can sometimes be important. But they are much more often a clue to something benign than a diagnosis of cancer on their own.
Do Breast Calcifications Cause Symptoms?
Usually, no. Breast calcifications typically do not cause pain, a lump, nipple discharge, or visible changes in the skin. They are usually silent and are found during routine breast imaging. That is one reason regular mammograms matter: they can detect tissue changes long before something becomes noticeable.
It is also worth knowing that mammography is the main tool for seeing calcifications. Ultrasound can help evaluate many breast findings, but many calcifications are not seen well on ultrasound. MRI is not the go-to test for spotting calcifications either. If calcifications are the issue, mammography usually takes center stage.
How Doctors Diagnose and Evaluate Breast Calcifications
Screening Mammogram
Most breast calcifications are first seen on a routine screening mammogram. If the calcifications look obviously benign, the radiologist may simply note them in the report and recommend normal screening going forward.
Diagnostic Mammogram
If the pattern is unclear or possibly suspicious, the next step is often a diagnostic mammogram. This is a more detailed mammogram that may include magnification views and additional angles. These images help the radiologist study the shape, number, and arrangement of the calcifications more closely.
A call-back for diagnostic imaging can be stressful, but it does not automatically mean cancer. Additional imaging is often a precaution, not a verdict. Most call-backs after screening mammograms do not end in a cancer diagnosis.
BI-RADS Category
Your mammogram report may include a BI-RADS assessment category. This system helps standardize how imaging findings are described and what follow-up is recommended.
- BI-RADS 1 or 2: Negative or benign finding
- BI-RADS 3: Probably benign; short-interval follow-up imaging is usually advised
- BI-RADS 4: Suspicious abnormality; biopsy should be considered
- BI-RADS 5: Highly suggestive of malignancy
For probably benign calcifications, repeat imaging may be recommended in 6 to 12 months, and sometimes continued for up to two years to confirm stability. If the calcifications change over time, the plan may change too.
Breast Biopsy
If the calcifications are suspicious, a biopsy may be recommended. When the target is visible mainly on mammography, doctors often use a stereotactic core needle biopsy. This method uses mammogram guidance to sample the exact area of concern.
The biopsy does not remove the entire breast lesion like surgery would. Instead, it collects tissue samples so a pathologist can examine them under a microscope. The goal is simple: determine whether the calcifications are benign, associated with high-risk changes, or related to cancer.
Treatment for Calcification in Breast
Treatment depends entirely on what the calcifications represent. The calcium itself is not the enemy. It is the underlying cause that drives the plan.
No Treatment Needed for Benign Calcifications
If the calcifications are clearly benign, no treatment is usually needed. You may simply continue your routine breast cancer screening schedule. In other words, the radiologist sees them, labels them harmless, and everyone goes home emotionally tired but medically relieved.
Short-Term Imaging Follow-Up
If calcifications are probably benign but not definitively harmless, your doctor may recommend a short-interval follow-up mammogram, often in about six months. This helps confirm that the pattern remains stable. Stability is reassuring. Change gets attention.
Biopsy-Based Treatment Decisions
If a biopsy shows benign tissue, you may need no further treatment beyond surveillance. If it shows atypical cells, DCIS, or invasive breast cancer, treatment is based on the diagnosis rather than the calcifications themselves.
Depending on the pathology report, treatment may include:
- Closer imaging surveillance
- Surgical removal of the abnormal area
- Radiation therapy
- Hormone therapy in selected cases
- Additional cancer treatment if invasive disease is present
For example, suspicious calcifications may lead to a biopsy that reveals DCIS. In that situation, doctors may recommend breast-conserving surgery, sometimes followed by radiation, depending on the extent and location of the abnormal cells. If invasive cancer is found, treatment may expand based on tumor type, stage, and receptor status.
When Should You Be Concerned?
You should not panic over the word “calcifications,” but you should pay attention to follow-up recommendations. Call your doctor or breast imaging center if:
- You were told to return for additional mammogram views
- Your report mentions suspicious or irregular microcalcifications
- You were advised to repeat imaging in six months
- A biopsy was recommended and you have questions about timing or results
- You also notice a new lump, skin change, nipple discharge, or breast pain that is unusual for you
The most helpful mindset is neither denial nor doom. Think of it as good detective work. The goal of breast imaging is to catch problems early and avoid missing subtle changes.
Can Breast Calcifications Be Prevented?
There is no proven way to prevent all breast calcifications because many occur as part of normal aging or benign tissue changes. Since they are not caused by dietary calcium, cutting out cheese is not the heroic move it might sound like. What does help is staying up to date with mammograms, knowing your personal breast cancer risk, and following through on recommended imaging or biopsy.
If you have a history of breast surgery, breast radiation, dense breasts, prior atypical biopsy findings, or a strong family history of breast cancer, talk with your clinician about the screening schedule that makes sense for you.
Frequently Asked Questions
Are breast calcifications usually cancer?
No. Most breast calcifications are benign. The concern rises when microcalcifications appear in suspicious shapes or clustered patterns.
Can calcifications in the breast go away?
Some may remain stable for years, while others may change over time. The key issue is not whether they disappear, but whether their pattern stays benign.
Can ultrasound detect breast calcifications?
Not reliably. Mammography is much better for detecting and evaluating calcifications.
Do all suspicious calcifications need surgery?
No. They often need a biopsy first. Surgery is considered only if the biopsy finds something that requires treatment.
Experiences Many People Have With Breast Calcifications
One of the most common experiences starts with total surprise. A person goes in for a routine mammogram feeling perfectly fine, leaves thinking about errands or lunch, and then gets a call saying additional images are needed because calcifications were seen. That call can feel huge, even when the actual finding turns out to be tiny. The emotional experience is often much larger than the physical one.
Many women describe the callback period as the hardest part. There is often no pain, no lump, and no obvious symptom to focus on, which oddly makes the imagination louder. People often say things like, “I felt normal, so how can there be something there?” That disconnect is common. Breast calcifications are usually an imaging finding, not something you can feel or notice day to day.
Another frequent experience is frustration with uncertainty. After a diagnostic mammogram, some people are told the calcifications look benign and they can return to routine screening. Others hear that the pattern is probably benign but should be checked again in six months. That six-month wait can feel emotionally inconvenient in the most deluxe way. It is short in medical terms and very long in human terms.
For people who need a stereotactic biopsy, the experience is often less dramatic physically than expected. Many report that the anticipation was worse than the procedure itself. There may be soreness, bruising, and anxiety, but the biopsy is usually done with local anesthesia and image guidance. The strange part for many is not the discomfort. It is the waiting for pathology results and wondering whether the word “calcifications” is about to become a much bigger story.
There are also many experiences of relief. A large number of people learn that their calcifications are benign and require no treatment. Others find out that the biopsy showed a high-risk lesion or DCIS rather than invasive cancer, which can still be overwhelming, but it also means the abnormality was found early. In that sense, calcifications sometimes become the clue that allowed early intervention before a lump ever developed.
Some people who have had previous breast surgery or radiation later learn that new calcifications are related to scar tissue, fat necrosis, or treatment effects. That can be reassuring, though doctors may still want imaging comparison or biopsy if the pattern is not classic. It is a reminder that the breast keeps a memory of what it has been through, and mammograms sometimes read that memory in bright white dots.
Emotionally, people often say they remember the wording of the callback more than the medical details. They remember where they were standing when the phone rang. They remember not hearing half the explanation because the words “come back” took over the room. That reaction is normal. It is also one reason clear communication from radiologists and clinicians matters so much.
In real life, the experience of breast calcifications is often a story about uncertainty, follow-up, and perspective. For some, it ends with reassurance. For others, it becomes the earliest sign of a problem that gets treated before it has a chance to grow. Either way, the experience teaches the same lesson: regular screening matters, patterns matter, and getting more information is not bad news by itself. Sometimes it is simply medicine doing exactly what it is supposed to do.
Conclusion
Calcification in breast tissue is common, often harmless, and usually discovered on mammography rather than through symptoms. The two main types are macrocalcifications and microcalcifications, and the biggest question is not whether calcium is present, but what pattern it forms. Benign causes include aging, cysts, fibroadenomas, prior inflammation, trauma, surgery, and vascular or skin changes. More suspicious patterns, especially clustered irregular microcalcifications, may point to DCIS or another breast abnormality that deserves closer evaluation.
When it comes to treatment, many people do not need any. Some need short-term imaging follow-up. A smaller group needs a biopsy, and treatment then depends on the pathology results. The bottom line is reassuring: breast calcifications are common, the majority are not cancer, and modern breast imaging is designed to sort the ordinary from the concerning with as much precision as possible.






